The Naso-gastric Sump Tube
So, you think you know about sump tubes.

Click the images to enlarge them.
What’s to know? Stick it in the stomach, hook it up to suction and let the weight of the suction tubing pull the blue and clear ends down below the patient. Right?

Wrong, if you want it to properly drain the stomach. And if you let the sump tube hang down like this, you may as well not put one in as it will probably not drain properly.
Why is it called a “sump tube” and not just a naso-gastric tube?
It is called a sump tube because it has two lumens. It is designed to overcome the problem of a single lumen tube; the sucking of the gastric mucosa or particulates into the tube’s stomach orifices (black arrows), which prevents removing the gastric contents.

If all of the orifices or merely the most proximal orifice gets plugged with food or mucosa, then the sump tube will stop draining the stomach.
Here’s how it is supposed to work: When the tube is properly inserted, and the clear plastic end attached to suction, air enters through the Luer-Lock filter and thence through the blue tubing into the stomach. Air entry into the stomach helps prevent the gastric mucosa from collapsing around the sump tube’s stomach orifices, which drain the stomach.

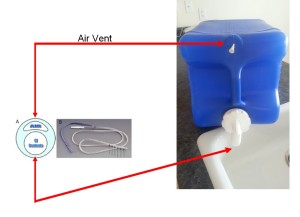
Air entry is key. For example, the blue water container will drain a lot better if the air vent is open. Keeping the air vent open is essential for the sump tube to drain properly.
To work properly, the Luer-Lock filter should be kept well above the patient’s stomach level.



If it falls below the level of patient’s stomach, gastric contents might drain back into the blue tubing, blocking the air entry, and defeating its purpose. If this happens, attach an air filled syringe to the Luer-Lock connector, flush the blue tubing with 10-15 cc of air, and secure the Luer-Lock filter orifice so that it is higher than the patient’s stomach. Additionally, you may have to flush the suction lumen with saline (30 – 50 ml) to dislodge what it is that is obstructing the suction lumen (food, mucosa). To do this, you will need a Foley catheter irrigation syringe.
Finally, you will have more success if you do NOT use full continuous suction, which is more likely to suck mucosa and food into the orifices. Low suction (up to 40 mm Hg) will produce better gastric drainage. You will have to remember to return the suction to FULL at the end of the operation in order to have adequate suction to clear the pharynx with the Yankauer.
These tubes are a nuisance to keep patent. When they are working properly, you can hear the sumping noise by listening at the Luer-lock filter orifice.
Do not do this…

when transporting the patient to the PACU or ICU.
The clear plastic connector (lower left) will be lost. Then, someone will open another sump tube package in order to replace the lost connector and they will discard an entire sump tube. What a waste!
Instead, transport the sump tube like this.


