Part of the Boeing 777’s check list:

I’m referring to the article “All That Glitters Is Not a Golden Recommendation” where Prielipp and Coursin1 condemn the guidelines supporting the peri-operative use of beta blockers for non-cardiac surgery, tight glyemic control in the ICU, and checklists. Although I agree with them that there has been adequate experience and time to criticize the value of beta blockers and tight glycemic control guidelines, I believe the jury is still out on checklists. Gawande published the “Checklist Manifesto”2 only 6 years ago and there has not been adequate time for their evaluation, especially since know-it-all doctors appear biased against them.
By juxtaposing the World Heath Organization’s (WHO) Universal Checklist (Figure 1) and the Landing Checklist for the Boeing 777 (Table 1) in their article, the authors imply that the WHO checklist is more complicated than that of the Boeing 777’s. Does this not speak to the authors own bias? This implication is simply not true. The WHO checklist is not a “landing checklist” but more akin to a “takeoff” checklist, which, for the Boeing 777, contains dozens upon dozens of checks.
See: http://www.atlanticsunairways.com/training/checklist_b777.pdf
The “takeoff” checklist for my single engine plane has 54 checks. Each check is important. Every time I think I can do it from memory I forget something making the takeoff perilous. I’ve always managed to salvage the precarious from memory takeoffs, and each time, I rue the fact that I didn’t do the checklist . One day, my occasional lack of diligence with the checklist could end with a takeoff crash.
To condemn checklists, the authors reference a Canadian study,3 which found “no difference in outcomes before and after the implementation of a checklist.” However the Editorial4 that accompanied that study, concluded, “The likely reason for the failure of the surgical checklist in Ontario is that it was NOT actually used.”
As I supervise multiple ORs, I always worry that we will one day operate on the wrong patient or the wrong side. I am thankful that our hospital has adopted a checklist similar to the WHO’s and I am amazed and thankful for how well our surgeons have bought into the process. We don’t “just check off boxes,” we actually “do what’s on the checklist.” In addition to preventing wrong patient or wrong side operations, the checklist introduces who is in the room and why they are there, reminds us of allergies, informs us as to what the surgeon is planning and what (s)he expects/needs from the OR staff, reminds us to administer antibiotics, and more.
It will be difficult to prove that checklists prevent complications. On the other hand, if checklists help us remember, say, to administer an antibiotic that might prevent an infection, that alone is valuable.
A reason commercial air travel is so much safer than hospitalizations is because pilots (unlike doctors) take checklists seriously. You don’t want to fly on an airline whose pilots are not rigorous about their checklists.
Addendum (Sept. 6, 2015):
What caught my attention most is that the author’s comments about the checklist did not rise to the same level of harm as with beta-blocker use and tight glycemic control. I think it is a stretch to lump the checklist with the other failures, especially since the checklist has not, in my opinion, been adequately shown to have failed (yet). In fact many articles seem to suggest that checklists are valuable (I have not done a rigorous review).
With the beta blockers and tight glycemic control guidelines, patients were harmed. I can not see how a checklist, in and of itself, would harm a patient.
The author’s focus is mostly on the POTENTIAL for checklists to disrupt teamwork and about being a zealous panacea for preventing complications, not so much for patient safety. I guess an unintended consequence of instituting a checklist could cause a dysfunctional group of healthcare providers to become more dysfunctional. In my opinion, instituting the checklist at our institution has fostered teamwork, not made it worse. As I said, I was amazed as to how our surgeons responded positively to its introduction/use.
The Boeing checklist is not used to foster teamwork or solve problems but to get the 777 off of the ground safely. There are only two people in the cockpit of a 777. If they can not work together, that is a real problem. If a checklist promotes teamwork, that is a plus, but I never saw that as important in any of the checklists that I use.
A checklist is merely an aid to keep me from forgetting something important. I have checklists for everything. One for running so that I don’t forget my gloves in winter, etc. One for when I am on call so that I don’t forget my cell phone, glasses, lunch, etc. Here is the one I pull up on the computer when I have a trauma:
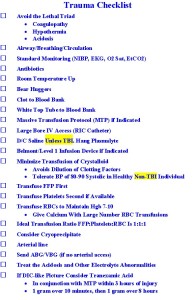
Trauma Checklist
There is chaos in a trauma. I pull it up as soon as I get word that the patient is coming or after I have stabilized the patient. This checklist merely focuses my attention and keeps me from forgetting something important.
No, a checklist will likely never be shown to STATISTICALLY prevent complications at the institutional level, but check this out:
If the pilots had done their checklist it would have made a NON-STATISTICALLY significant difference to them and their 5 passengers, all of whom died.
Addendum (Sept. 13, 2015)
According to the NTSB’s final report, “The pilots of the Gulfstream were experienced and had flown the plane together many times, but records showed almost never performed basic safety checks.“
The corollary is that the pre-procedure checklist can prevent accidents in the OR. “Know-it-all-doctors who believe they don’t need a checklist might take heed and learn from this tragic jet crash.”
REFERENCES
- Prielipp RC, Coursin DB. All That Glitters Is Not a Golden Recommendation. Anesth Analg 2015;121: 727-33
- Gawande A. The Checklist Manifesto: How to Get Things Right. New York, NY: Metropolitan Books, Henry Holt and Company, LLC, 2009
- Urbach DR, Govindarajan A, Saskin R, Wilton AS, Baxter NN. Introduction of surgical safety checklists in Ontario, Canada. N Engl J Med 2014;370:1029–38
- Leape LL. The checklist conundrum. N Engl J Med 2014;370:1063–4
LINKS
All That Glitters Is Not a Golden Recommendation
Surgical Safety Checklists in Ontario
Checklist Conundrum



